
Recently, as a doctor working in the ICU tending to patients who’ve been operated, I was caught between the devil and the deep sea. I was involved in the treatment of a 51-year old lady who had received treatment in various hospitals for pancreatic cancer, for which her family had already spent a fortune. She had come to us for surgical rectification of a complication that had arisen as fallout of an operation she had undergone earlier. Not in the best of health, having been in and out of hospital for quite some time, she was not in an ideal physical condition to undergo another major surgery, which was however imperative. After surgery she suffered a setback on the form of heart failure, which almost placed her at death’s door. Prompt intervention including ventilation saw her improving over subsequent days, much to her treating doctors’ gratification.
Just as we thought that she was turning the corner, her husband demanded that all treatment be withheld. He claimed to have ‘exhausted all resources treating his wife for years’. Though it was a tough decision, which he was guilty about, he had no option but to give up on his wife for want of money.
His request to ‘pull the plug’ on his wife who was improving had her treating team disappointed as well as taken aback. We were torn between a patient who was improving to treatment from near-death and her husband who wanted treatment for his wife stopped, because he didn’t have the money, which if complied with meant certain death.
This isn’t an isolated incident played out in hospitals. Modern Medicare isn’t cheap anymore. It inflicts huge financial burden on families, irrespective of their financial wherewithal. While healthcare personnel go about the difficult preposition of treating patients who need to surmount many an odd, their families run from pillar to post raising money to pay mounting bills. In India where healthcare insurance does not measure up to patients’ needs, doctors are often asked to ‘stop treatment’, which could be easily complied with in patients who’re over the hill, for whom treatment is futile, but is a catch twenty two situation in a patient like the one I was involved in treating. Medical personnel, hospital managements and the government need to put their heads together to promulgate measures that would make the very prospect of treating diseases less cumbersome, especially for families of those patients who are improving to treatment, and lack the financial clout to take treatment to its entirety.
Continuing with the story of the patient I had mentioned above, she took a downhill course the very next day, with her liver and kidneys playing up. The husband, who only the other day chose to suspend treatment for his wife, saw a window of opportunity in the worsening of her condition the next day to lob the ball back into the doctors’ court. He burdened the doctors to take ‘suitable’ decision for his wife who had deteriorated overnight. The doctors couldn’t run away from the tight corner they found themselves in. He cleverly turned the tables on them to ‘do whatever is best for the patient’, which was exactly incongruent to the stand he had taken only the previous day, when he wanted all treatment stopped for his wife. As the day wore on, he reached the height of his predicament over his wife’s treatment, which had drained him financially. Citing inability to afford continuation of treatment, his dillydallying had him arm-twist us to remove his wife from the ventilator, knowing perfectly well that the outcome would be sure death, which he was ready to face anyway. Almost soon after she was taken off the ventilator, he wanted his wife to be moved from the ICU to the room, simply because he was in dire financial straits. This kind of extreme requests from the immediate dear and near of patients are typical in the face of severe financial stress. As expected, the patient passed away the same night. Though the husband might seem ‘cruel’, we perfectly empathized with his painful situation.
Aren’t there ways and means whereby families who find money hard to come by are able to provide affordable, yet effective treatment for their near and dear?
- Statistically, healthcare facilities in the public sector far exceed those in the private sector, especially those in the corporate sector by sheer number. Those in the government sector provide much cheaper healthcare than those in the private sector. As the result, it is to the former that a large number of India’s sick, especially those belonging to the economically wanting section of society approach seeking medical care. Paradoxically, ‘cheaper facilities’ existing in public hospitals are unable to measure up to the quality of treatment provided in private facilities. This is not entirely due to the paucity of facilities alone. There is a glaring incongruity between work culture that exists among the personnel manning healthcare facilities in the public and private healthcare facilities. While ‘work to rule’ work ethics is the rule in government facilities, healthcare workers in the private sector are ready to walk that extra mile for patients, especially the sicker ones, who demand dedicated and undivided attention. This must change. Besides, there is prominent paucity of facilities and advanced technology that aid both in diagnostic and therapeutic purposes in the public sector. The common excuse citied for the government healthcare facilities lacking adequate facilities is ‘paucity of funds with the government’. Healthcare isn’t a priority for the government, which only spends less than 1% of the GDP for healthcare dispensation. To circumvent dependence on government funds to spruce up public healthcare facilities to which the poor approach for their health needs, a viable option is to levy menial consultation fees for just outpatient consultations alone in the government hospitals. States like Kerala which has significant leftist political influence had once attempted to do this, but had to backtrack, as it was met with determined opposition from left-leaning political forces. It will take a committed political will to put this in place. Considering the humongous numbers of patients seeking outpatient consultation in public hospitals, the kind of money that can be generated from a menial fee could be substantial enough to fund the respective hospitals’ modernization. If people willingly spent huge amounts of money on booze and cigarettes, which only spell doom on their health, it is also their responsibility to spare some money for their health needs. Politicians fight attempts to charge services in public hospitals for their narrow-minded political gains. Monitory self-sufficiency alone can pull public healthcare sector from the depths of dismal existence in apparent squalor.
- Healthcare in India is greatly handicapped by lack of a buoyant insurance industry, as that exists in the West. Though there are large numbers of agencies offering ‘health insurance’ to the public, they are known to foot-drag on processing claims and even refuse disbursement of claims which the insured rightfully deserve for the premium paid on insurance. Insurance companies look out for loopholes or excuses to withhold disbursement of claims, on flimsy excuses taking the insured for a ride. This sector need to be pulled up and regulated, as medical insurance is, on many occasions, the only source of money people, especially the insured (theoretically) have to fall back on, to pay hospital bills. The insured must at least be provided a platform to voice their grievances on the insurance companies’ highhandedness.
- Those employed with government and their dependents have the facility wherein medical expenses incurred are reimbursed. It cannot be denied that this facility is of great help for government servants and their dependents. On many occasions, this facility is entangled in the red tape. This facility must be made less cumbersome in living up to the financial needs of those who are entitled beneficiaries of this truly humanitarian facility, in times of great financial stress caused by medical needs.
- As things exist, private healthcare facilities, especially those in the corporate sector indulge in runaway ‘exhortation’ by fleecing the unfortunate sick who have no option but to cough up money to pay the long bill that props out of billing machines in private hospitals. If there is one segment of healthcare the government needs to shackle is the inhuman fleecing of patients in the name of billing indulged in by private hospital managements. The government must also attempt to do away with the practice among private hospitals to demand money as ‘advance’ when patients are admitted to hospitals. This practice is inhumanly followed even in emergencies like road traffic accidents. No person who meets with an accident is expected to land up in hospitals with bloated wallets!
- Doctors and hospitals must be more forthcoming to oblige to patients’ or their families’ requests for transfer to cheaper healthcare facilities of their choice, if that will help reduce treatment costs.
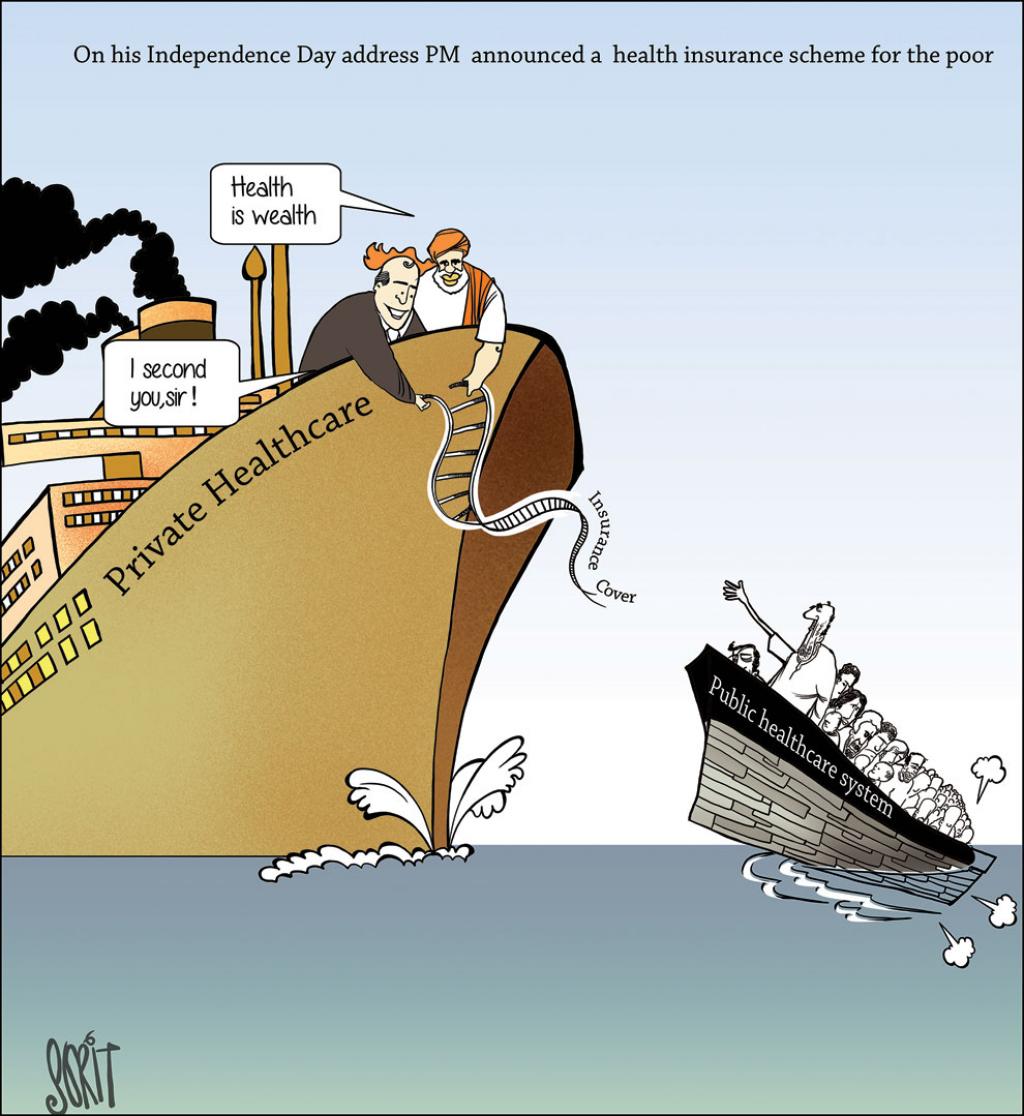
- Government schemes like the ambitious Ayushman Bharat Yogana free Health Insurance Scheme, the brainchild of the incumbent Prime Minister Narendra Modi will go a long way to address the financial aspects associated with healthcare needs of the nation’s citizens, especially those who are financially hard-pressed. More such schemes are truly welcome
- Charity by well-meaning individuals, organizations and clubs must also be encouraged, but with stringent regulation and screening of the needy. Group funding will also go long way to mitigate the financial hardship caused by costly medical needs. Requests through media, both the print and visual are sometimes resorted to by people who have their back to the wall, having lost their worldly possessions in the process of paying up hospital bills. But, such efforts are sometimes resorted to by unscrupulous elements as means to cheat people to make easy money! Such self-defeating attempts must face the long arm of the law.

Leave a comment